by DAVID BROWN | CLEARNFO.com | December 26, 2021
As the COVID saga continues, it is undeniable the officially promulgated numbers are confused, conflicted and unreliable. In the beginning, many of us took the official numbers at face value. The media’s narrative was and is driven primarily by the number of ‘cases’ and sometimes misattributed deaths; yet few of us know the finer details behind these frightening headlines. Seemingly, simple questions like: “What is a case?; What is a COVID death?; What is COVID pneumonia?; What does it mean to test positive if you have no symptoms and how accurate are the PCR tests amplified at 40 cycles looking only at three small segments (RdRp, S & N) of a proposed virus in silico?” Answers to these questions remain elusive, nondeterministic and subject to interpretation and manipulation.
One would think a case is a confirmed COVID infection, but this is just not so. We learn a case can be suspect, probable, or confirmed and even the confirmed cases cannot be confirmed with the formally gold standard test. The definitions of case categories represent a long and winding road of updates and links to other definitions; all subject to change at the whim of the experts. Add to this, long established definitions of key terms like vaccine, herd Immunity and pandemic have been quietly altered since COVID.
Note: with the advent of the COVID-19 project, the term vaccinated became ‘fully vaccinated’ and is now called ‘up to date’. Add to this, if you have had two doses of the mRNA injections, you are considered ‘unvaccinated’ until 14 days after your second dose; and even then you are faced with potentially unlimited booster shots every few months to maintain your up to date status; thus you are unvaccinated if you are not up to date. These moving targets can add to the already hot mess found in the faulty data collection and analysis.
Yet, we constantly hear about the incredible number of cases, while few if any know what a case is. What is a case? Ask any doctor, media pundit or health professional this question and you are likely to get a blank, confused stare. They may think you are an idiot because everyone knows what a case is, but they don’t.
We are told the CDC’s own VAERS database –designed to track adverse events– is not accurate; we have collected this information every year since 1990 for what purpose if it is unreliable?
So what are the real numbers? We will never know, but we can attempt to come up with a rough order of magnitude using the information we have to date.
Since March of 2020, I talked with many health professionals who had no idea what VAERS was; or, that they should be reporting these adverse events in the VAERS database. It takes time and effort to make even one entry, and many who know about VAERS just don’t take the time; so it is my personal opinion the adverse events are hugely underreported. But what does the latest VAERS show us? See the so called ‘Harvard’ VAERS study below. Be careful not to call it a ‘Harvard study’ lest you be attacked by a swarm of paid fact-checkers.
“It is worth pointing out that Harvard Pilgrim Health Care, Inc., has no affiliation with Harvard University. Electronic Support for Public Health–Vaccine Adverse Event Reporting System (ESP:VAERS)” https://digital.ahrq.gov/sites/default/files/docs/publication/r18hs017045-lazarus-final-report-2011.pdf
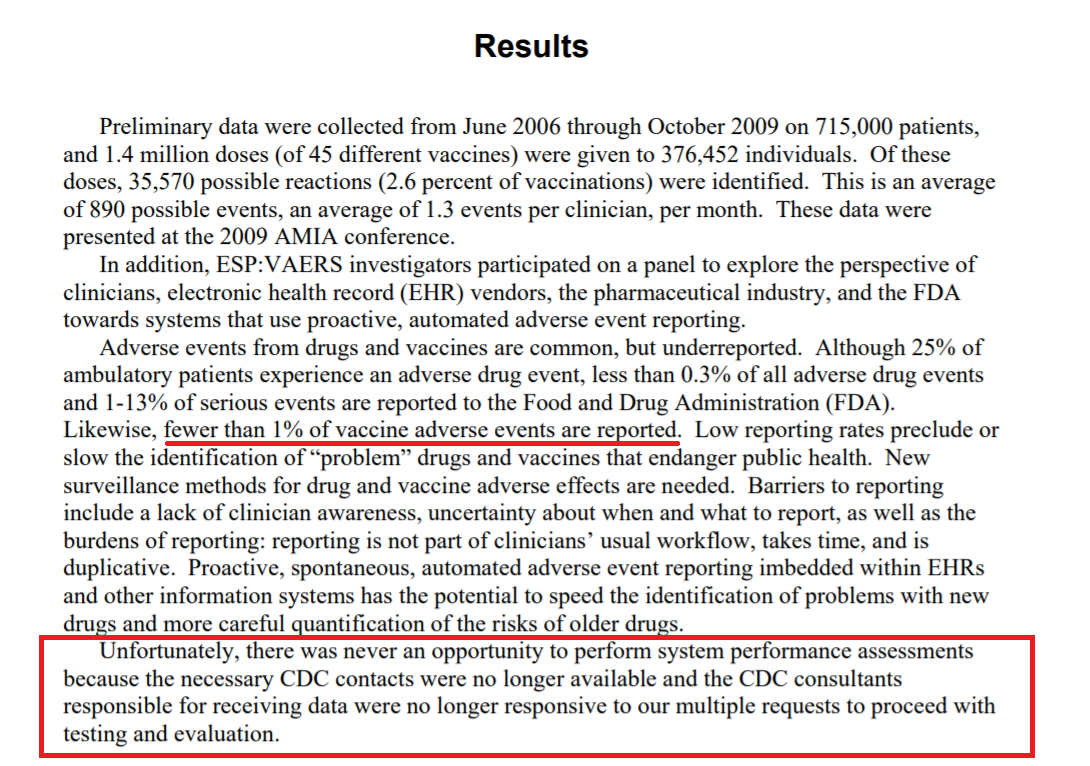
The Pilgrim Health Care, Inc. study (sometimes called the Harvard study) does point us in the direction of under-reporting in VAERS by a factor of 100X; but even at 10X, these figures are breathtaking. If these numbers are correct, we are looking at a mass genocide of historical proportions, while our trusted experts continue to pretend these injections are ‘safe & effective’. This does not include any mid to long-term damage from this global experiment.
The CDC’s VAERS shows there have been 983,756 reports of vaccine adverse events; 34,615 permanently disabled 3,365 Miscarriages, 10,429 heart attacks and 20,622 reported deaths through December 17, 2021. Source: https://openvaers.com/covid-data
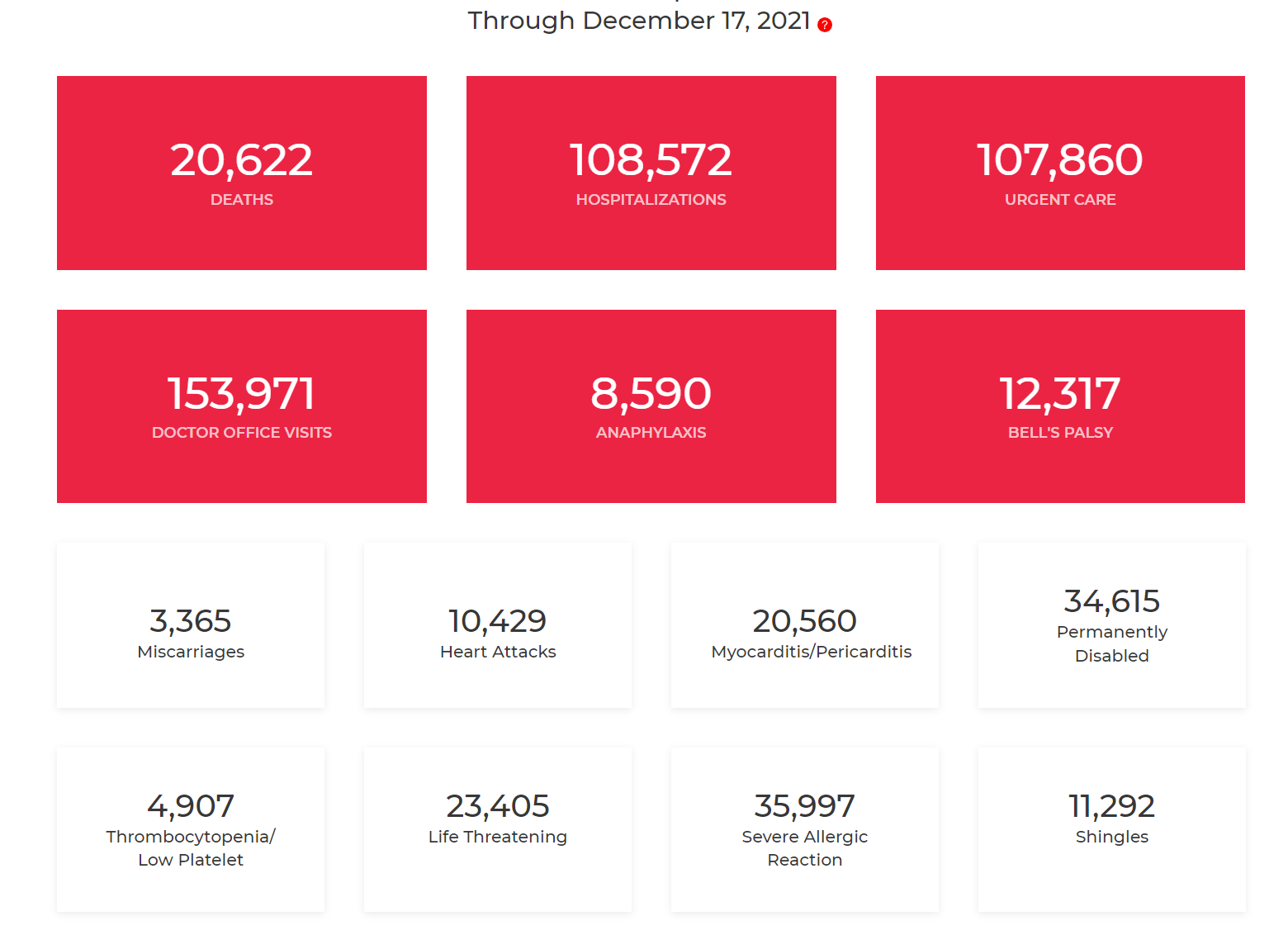
These figures may not be accurate but a comparison of previous years, may be instructive since they dwarf all other records kept since 1990: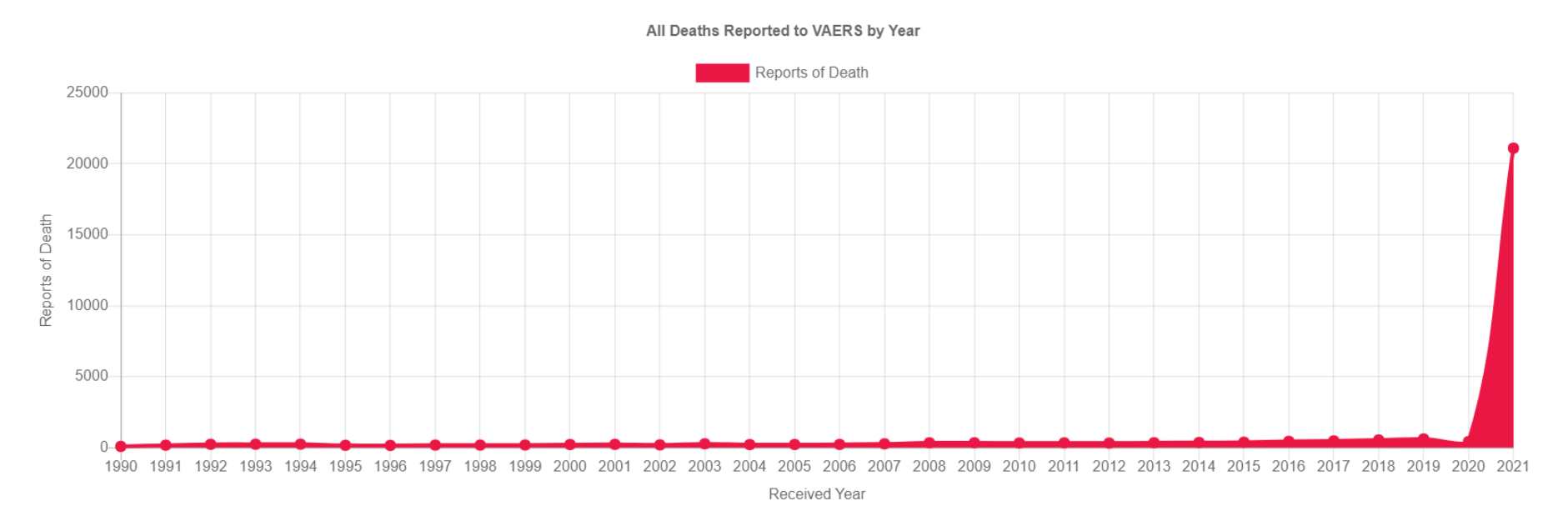
As of December 23, 2021 we are told the total number of COVID deaths is 808,957, yet we discover most of these deaths were unnecessary: “Of the COVID-19 deaths in the U.S., none received adequate and/or early-enough treatment. At least 85% of COVID deaths were preventable.” Source: https://childrenshealthdefense.org/defender/covid-deaths-could-have-been-prevented/
This means 687,613 people were needlessly killed by withholding early treatment.
Additionally, we discover those who were unlucky enough to be admitted to the hospital after their lips turned blue, were given the deadly Remdesivir known to cause kidney failure which then causes their lungs to fill with fluid, so the hospitals could put them on a vent to die. This means the officially sanctioned protocol is killing most of the people, not the dreaded, scary COVID; yet the CDC and others get to report 808,957 died of COVID which is just not true.
So what are the real numbers?
To be generous, 121,343 may have died from COVID. But the question remains: Of these 121,343 how many died with COVID and how many died from COVID? How many died from some comorbidity or even as a result of an unrelated accident? We will never know.
And what is a case? There is no clear definition I can find. The more I read about the definition of a case the more murky it becomes, but I’ll let you decide.
END
References & Additional Reading:
Alberta just inadvertently confessed to fiddling the COVID vaccination stats. More than half the newly vaccinated deaths were dumped in the unvaccinated. –Joel Smalley
All-Cause Mortality: COVID-19: FOLLOWING THE MONEY | The Highwire with Del Bigtree
Remdesivir with Dr. Bryan Ardis:
https://dailyexpose.uk/2021/09/02/remdesivir-causes-renal-failure-hospital-protocols-are-killing-people/
The so called Harvard VAERS study: It is worth pointing out that Harvard Pilgrim Health Care, Inc., has no affiliation with Harvard University. Electronic Support for Public Health–Vaccine Adverse Event Reporting System (ESP:VAERS) https://digital.ahrq.gov/sites/default/files/docs/publication/r18hs017045-lazarus-final-report-2011.pdf
VAERS, Underreporting, and the Mysterious 1% https://gnigh-66270.medium.com/vaers-underreporting-and-the-mysterious-1-5b4f9b109145
US COVID-19 cases and deaths by state https://usafacts.org/visualizations/coronavirus-covid-19-spread-map/
What is a case? https://ndc.services.cdc.gov/case-definitions/coronavirus-disease-2019-2021/
PCR test and how conducted by Chris Martenson @ Peak Prosperity starting at 4:51 minutes in. Omicron Deaths – A Surprising Number Premiered Dec 22, 2021 https://www.youtube.com/watch?v=0Su878hS_wg
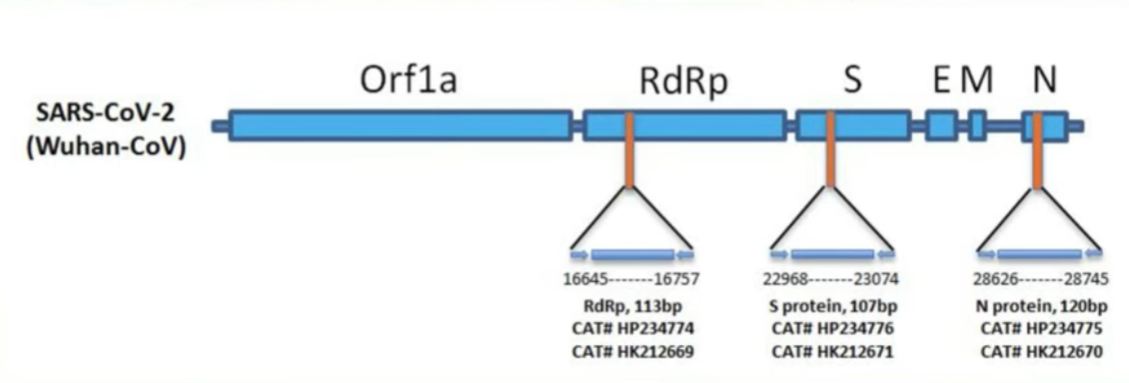
Looking for three parts with the PCR test: 1) RdRp; 2) S; 3) N
Swab up nose; Take RNA and amplify (40 cycles?); They take a little stretch or parts to see if they match.
WHO Variants of concern: https://www.who.int/en/activities/tracking-SARS-CoV-2-variants/
- Alpha (B.1.1.7) – September 2020 in UK
- Beta (B.1.351) – South Africa May 2020
- Gamma (P.1) – Brazil November 2020
- Delta (B.1.617.2) – India October 2020
- Omicron (B.1.1.529) – Multiple countries November 2021
Story at-a-glance: Source: https://childrenshealthdefense.org/defender/covid-deaths-could-have-been-prevented/
- Of the COVID-19 deaths in the U.S., none received adequate and/or early-enough treatment. At least 85% of COVID deaths were preventable.
- There are three components to SARS-CoV-2 infection: viral replication, cytokine storm and blood clotting, therefore necessitating a multidrug approach, and treatment must begin early to be effective.
- Research published in 2006 showed hydroxychloroquine reduced viral replication of SARS-CoV-1 (the original SARS virus). It also has well-established anti-inflammatory properties. These two properties help explain its usefulness against COVID-19.
- There were clear intentional efforts to prevent use of hydroxychloroquine against COVID-19, likely in an effort to make the COVID jabs appear necessary.
- You cannot get COVID-19 twice — those with natural immunity have robust, long-lasting immunity. The Pfizer COVID shot, meanwhile, has been shown to have undetectable effectiveness 201 days after the second dose and Moderna’s effectiveness reaches zero around day 121.
PREP Act: Public Readiness and Emergency Preparedness Act https://en.wikipedia.org/wiki/Public_Readiness_and_Emergency_Preparedness_Act
EUA Emergency Use Authorization: https://en.wikipedia.org/wiki/Emergency_Use_Authorization
Dr Ardis Remdesivir: https://thedrardisshow.com/
Doctor Reveals Remdesivir Is Real Cause Of COVID-19 Maladies
Doctor Reveals Remdesivir Is Real Cause Of COVID-19 Maladies
Way Back Machine (Web Archive): Remdesivir
Last Updated: May 12, 2020 Recommendations: https://web.archive.org/web/20200604123510/https://www.covid19treatmentguidelines.nih.gov/antiviral-therapy/remdesivir/
Hospitals Are Paid Federal Cash For Every COVID-19 Patient They Admit & Even More If You Die Of It Basically it’s state sponsored murder
Hospitals Are Paid Federal Cash For Every COVID-19 Patient They Admit & Even More If You Die Of It
NIH New Treatment Guidelines updated December 16th, 2021 (Credit NIAID-RML) : https://files.covid19treatmentguidelines.nih.gov/guidelines/covid19treatmentguidelines.pdf
Midazolam: Midazolam, sold under the brand name Versed, among others, is a benzodiazepine medication used for anesthesia, procedural sedation. Midazolam can slow or stop your breathing, especially if you have recently used an opioid medication or alcohol. Midazolam is given in a hospital, dentist office, or other clinic setting where your vital signs can be watched closely. https://www.drugs.com/mtm/midazolam.html
Isolated virus? Has SARS-COV-2 been isolated and purified to show existence?
AUGUST 21, 2021 ALGORA BLOG 1 COMMENT
Koch’s postulates Stew peters show where’s covid https://www.bitchute.com/video/bqghf9wOc7aM/
http://hedrick.ucsd.edu/BICD136/Lectures/Lecture16-Denialists.pdf
Robert S. Mendelsohn temple of doom : http://whale.to/a/hospitals1.html
What is a COVID Case from CDC… https://www.cdc.gov/coronavirus/2019-ncov/covid-data/faq-surveillance.html
A COVID-19 case is an individual who has been determined to have COVID-19 using a set of criteria known as a case definition. Cases can be classified as suspect, probable, or confirmed. CDC counts include probable and confirmed cases and deaths. Suspect cases and deaths are excluded.
The case classifications for COVID-19 are described in an updated interim COVID-19 position statement and case definition issued by the Council of State and Territorial Epidemiologists. A probable case or death is defined as any one of the following:
Meets clinical criteria AND epidemiologic linkage with no confirmatory laboratory testing performed for SARS-CoV-2
Meets presumptive laboratory evidence
Meets vital records criteria with no confirmatory laboratory evidence for SARS-CoV-2
Any cases and deaths classified as probable are included in CDC case counts. The same applies to any cases and deaths classified as confirmed.
The Centers for Disease Control and Prevention (CDC) will no longer recommend its PCR test to detect the CCP virus, saying that it will withdraw the test’s emergency use authorization (EUA), and instead, encourage labs to use a multiplex assay that can detect and differentiate the virus from the flu.
“Given the availability of commercial options, CDC intends to discontinue support for the CDC 2019 Novel Coronavirus (2019 nCoV) Real-Time RT-PCR Diagnostic Panel, the assay first introduced in February 2020 for detection of SARS-CoV-2,” Jasmine Reed, public affairs specialist at the CDC, told The Epoch Times via email.
She added that “… the demand for this test has declined with the emergence of other higher-throughput and multiplexed assays. CDC is encouraging pubic health laboratories (PHL) to adopt the CDC Influenza SARS-CoV-2 (Flu SC2) Multiplex Assay to enable continued surveillance for both influenza and SARS-CoV-2, which will save both time and resources for PHL.”
The public health agency said its multiplex assay had been granted an emergency authorization last year in July 2020 and describes it as a “real-time reverse-transcription polymerase chain reaction (RT-PCR) test that detects and differentiates RNA from SARS-CoV-2, influenza A virus, and influenza B virus in upper or lower respiratory specimens” from individuals in the acute phase of infection
CDC to Replace Its PCR Test With One That Can Differentiate Between CCP Virus and Flu
JUL 28, 2021
Source: https://yournews.com/2021/07/28/2189477/cdc-to-replace-its-pcr-test-with-one-that-can/
Christian Perronne Testimony at the Luxembourg Parliament – At the Parliamentary hearing in Luxemburg January 12, 2022.